

-
 By:
Valerie Puffenberger, PMHNP-BC
By:
Valerie Puffenberger, PMHNP-BC
-
 Editor:
Phyllis Rodriguez, PMHNP-BC
Editor:
Phyllis Rodriguez, PMHNP-BC
-
 Clinical Reviewer:
Dr. Ash Bhatt, MD, MRO
Clinical Reviewer:
Dr. Ash Bhatt, MD, MRO
Medication-assisted treatment has fundamentally changed what is possible in opioid use disorder recovery. Where decades of treatment philosophy insisted that medications were simply a replacement for one dependence with another, the clinical evidence has been clear and consistent for years: buprenorphine-based medications reduce cravings, prevent withdrawal, lower overdose risk, and significantly improve long-term recovery outcomes.
The question today is no longer whether medication-assisted treatment works. It is which medication, for which person, at which stage of their recovery, and why.
Sublocade and Suboxone are both buprenorphine-based medications approved by the FDA for the treatment of opioid use disorder. They share the same active ingredient and the same fundamental mechanism of action. But how they are administered, how they work in the body, and which patients they serve best are meaningfully different, and those differences matter clinically.
This guide is designed to give patients, families, and anyone navigating the question of MAT a clear, honest, and clinically grounded understanding of both options.
Key Takeaways1. Both medications work, but they work differently. Sublocade and Suboxone share the same active ingredient but differ fundamentally in how they are delivered, how they behave in the body, and which patients they serve best. Understanding those differences is the starting point for any good MAT decision. 2. Adherence is where many MAT programs succeed or fail. Sublocade’s monthly injection eliminates the daily dosing requirement that causes many patients to miss doses, struggle with diversion risk, or experience breakthrough cravings. For patients with adherence challenges, this pharmacological advantage is clinically significant. 3. The medication is only part of the answer. The evidence is consistent: MAT combined with behavioral therapy and clinical support produces better outcomes than medication alone. A comprehensive program, not just a prescription, is what lasting opioid recovery requires. |
What Is Sublocade?
Sublocade is the brand name for extended-release buprenorphine, administered as a subcutaneous injection, a shot delivered just beneath the skin of the abdomen once per month. It was approved by the FDA in 2017 and represents a significant advancement in buprenorphine delivery: rather than requiring daily doses, Sublocade forms a solid deposit under the skin that releases buprenorphine steadily over approximately 28 days.
It is prescribed exclusively by certified healthcare providers and administered in a clinical setting, it cannot be self-administered. This distinction has important implications for both adherence and treatment structure, which we will explore below.
How the Monthly Injection Works
When Sublocade is injected subcutaneously, the liquid formulation solidifies almost immediately into a small depot, a firm, pea-sized mass beneath the skin. From this depot, buprenorphine is released at a consistent, controlled rate throughout the month. Blood levels of buprenorphine rise gradually after injection, reach a therapeutic plateau, and remain relatively stable until the next injection.
This pharmacokinetic profile, steady, predictable medication levels rather than daily peaks and troughs, is one of Sublocade’s defining clinical advantages. Stable buprenorphine levels mean consistent craving suppression and consistent opioid receptor occupancy, leaving little window for the kind of breakthrough cravings that can occur between daily doses of oral medications.
| How Sublocade differs pharmacologically:
• Administered once monthly by a clinician – no daily dosing • Forms a subcutaneous depot that releases buprenorphine steadily • Produces stable, consistent blood levels throughout the month • Cannot be diverted, shared, or misused – always clinician-administered • Available in two doses: 100mg and 300mg monthly |
Benefits of a Long-Acting Buprenorphine Option
Elimination of daily dosing burden. For many people in recovery, the daily ritual of taking medication can itself become a source of anxiety, temptation, or missed doses. Sublocade removes that daily decision entirely.
No risk of diversion or misuse. Because Sublocade is administered only in a clinical setting, there is no medication to take home, share, sell, or misuse. This is particularly significant for patients whose home environments present risks to recovery.
Consistent therapeutic coverage. Stable blood levels throughout the month mean consistent craving suppression, no gaps, no peaks and troughs, no windows of vulnerability tied to dosing schedules.
Structured clinical contact. Monthly injection appointments create a natural cadence of regular clinical check-ins, supporting accountability and allowing providers to monitor progress consistently.
Reduced stigma of daily medication. For patients who find daily sublingual dosing socially uncomfortable or stigmatizing, a once-monthly injection offers a more discreet and less frequent treatment experience.
Common Side Effects of Sublocade
Sublocade is generally well tolerated. The most commonly reported side effects are localized to the injection site and include redness, itching, pain, or the presence of a firm depot mass under the skin, which resolves over time as the medication is absorbed. Systemic side effects are consistent with buprenorphine generally and may include constipation, nausea, headache, and fatigue, particularly in the days following injection.
Because Sublocade cannot be dose-adjusted once administered, patients should discuss any concerns about dosing with their provider before each injection.
What Is Suboxone?
Suboxone is the brand name for a combination of buprenorphine and naloxone, available as a sublingual film or tablet that dissolves under the tongue. It has been approved by the FDA for opioid use disorder treatment since 2002 and remains one of the most widely prescribed medications in addiction medicine.
Unlike Sublocade, Suboxone is prescribed for self-administration, patients take their daily dose at home, dissolving the film under the tongue. This flexibility makes it the more common starting point for opioid use disorder treatment, particularly during the induction phase when doses are being calibrated.
How Suboxone Works in the Brain
Suboxone contains two active ingredients that work together. Buprenorphine is a partial opioid agonist, it binds to the brain’s opioid receptors and activates them, but with a ceiling effect that limits the degree of euphoria and respiratory depression compared to full agonists like heroin or oxycodone. This partial activation is enough to suppress withdrawal symptoms and cravings without producing the kind of high associated with misuse.
Naloxone, the second ingredient, is an opioid antagonist, it blocks opioid receptors and is included primarily as a deterrent to injection misuse. When Suboxone is taken as directed (dissolved under the tongue), the naloxone has minimal systemic effect. If someone attempts to inject it, the naloxone becomes active and precipitates withdrawal, a powerful disincentive to misuse.
“Buprenorphine’s ceiling effect is one of its most important safety features it dramatically reduces the risk of overdose compared to full opioid agonists, even at higher doses.”
Benefits of Flexible Daily Dosing
Dose adjustability. Suboxone can be titrated up or down in response to a patient’s clinical needs, particularly valuable during induction and in the early weeks of treatment when the right dose is being established.
Established long-term evidence base. With over two decades of clinical use, Suboxone has an extensive evidence base supporting its effectiveness across diverse patient populations and treatment settings.
Accessibility and availability. Suboxone is widely available at pharmacies across the United States and is covered by most insurance plans and state Medicaid programs.
Appropriate for early treatment. The flexibility of daily dosing makes Suboxone the preferred option during induction, the initial phase of MAT when the correct dose is being identified.
Common Side Effects of Suboxone
Suboxone is generally well tolerated, particularly once an appropriate dose is established. Common side effects include headache, nausea, constipation, sweating, insomnia, and oral numbness or irritation from sublingual administration. As with all buprenorphine formulations, patients should avoid taking Suboxone alongside benzodiazepines, alcohol, or other central nervous system depressants, as these combinations increase respiratory risk.
Patients who miss doses may experience breakthrough withdrawal symptoms, one of the primary clinical limitations of daily oral formulations compared to the steady-release profile of Sublocade.
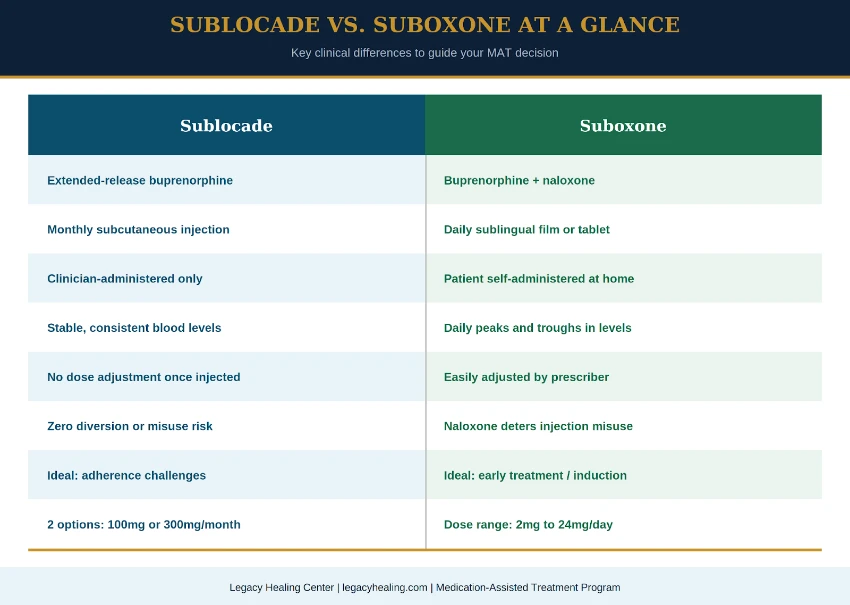
The Difference Between Sublocade and Suboxone
Understanding how these two medications differ across key clinical dimensions is essential to making an informed treatment decision. The table below summarizes the most significant distinctions.
Effectiveness for Opioid Use Disorder
Both Sublocade and Suboxone are evidence-based, FDA-approved treatments with demonstrated effectiveness in reducing opioid use, preventing relapse, and supporting long-term recovery. The clinical evidence for buprenorphine-based MAT overall is among the strongest in addiction medicine.
Clinical trials for Sublocade demonstrated significantly higher rates of opioid-negative urine samples among participants receiving the injection compared to placebo. Importantly, the controlled-release formulation produced consistently higher minimum buprenorphine blood levels than typical oral dosing schedules, a pharmacological advantage that translates clinically into more consistent craving suppression.
Suboxone’s effectiveness across more than two decades of clinical use is well established. It significantly reduces illicit opioid use, decreases overdose mortality risk, improves treatment retention, and reduces the social and economic costs associated with untreated opioid use disorder. Combined with behavioral therapies, which we at Legacy Healing integrates into every MAT program, outcomes improve further.
| What the research tells us:
• Buprenorphine-based MAT reduces opioid use by 50% or more in most clinical studies • MAT combined with behavioral therapy produces better outcomes than either alone • Treatment retention, staying in treatment, is one of the strongest predictors of long-term recovery • Both Sublocade and Suboxone significantly reduce overdose mortality risk compared to no treatment • Extended-release formulations may improve treatment retention through elimination of daily adherence demands |
Is Sublocade Better Than Suboxone?
This is one of the most common questions patients and families ask, and it deserves a direct, honest answer rather than a clinical non-answer.
For certain patients, Sublocade is clearly the superior clinical choice. If someone has struggled with medication adherence, has a history of relapse during treatment, lives in an environment where daily medication management is difficult, or has reached a stable phase of recovery and wants to simplify their treatment, Sublocade’s once-monthly profile addresses those specific challenges in a way that daily Suboxone cannot.
For other patients, particularly those in the early induction phase, those who require frequent dose adjustments, or those for whom the cost difference is a material barrier. Suboxone remains an excellent, and clinically appropriate choice.
“There is no universally better option. There is only the better option for this patient, at this stage of their recovery, given their specific clinical picture. That determination should always be made with a qualified addiction medicine specialist.”
Can You Switch From Suboxone to Sublocade?
Yes, and for many patients, this transition represents a meaningful step forward in their recovery. Sublocade is designed to be initiated after a patient has already been stabilized on a sublingual buprenorphine product such as Suboxone.
“Patients already receiving 8–24mg daily of transmucosal buprenorphine may transition directly to Sublocade on the same day. Patients not currently on buprenorphine must first receive a test dose (e.g., 4mg) of oral buprenorphine and be monitored for one hour to confirm tolerability before receiving the first injection.”
The transition itself is typically straightforward when managed by an experienced addiction medicine provider. The first Sublocade injection is administered after the final sublingual dose. Patients may experience mild withdrawal symptoms in the first few days after the initial injection as blood levels are still rising. This is normal and expected, and providers should discuss this with patients in advance.
Cost and Insurance Coverage
Cost is a real and legitimate consideration in MAT decisions, and one that deserves a straightforward conversation rather than being dismissed or minimized.
Cost of Sublocade
Sublocade carries a higher list price than oral Suboxone, typically ranging from $1,500 to $1,900 per monthly injection at list price before insurance. However, the manufacturer (Indivior) offers a patient assistance program for eligible uninsured or underinsured patients, and many commercial insurance plans cover Sublocade, particularly following the expansion of MAT coverage under the Affordable Care Act’s mental health parity provisions.
At Legacy Healing, our admissions and insurance team can verify coverage quickly and clearly before treatment begins.
Cost of Suboxone
Brand-name Suboxone is more expensive, but generic buprenorphine/naloxone films and tablets are widely available and significantly reduce out-of-pocket costs. Most commercial insurance plans and state Medicaid programs cover buprenorphine/naloxone formulations, making Suboxone and its generics broadly accessible.
The indirect costs of daily medication management, pharmacy visits, time, and the cognitive and emotional weight of daily dosing, are real but less frequently accounted for in cost comparisons. Some patients find that Sublocade’s once-monthly structure ultimately reduces the overall burden and indirect costs of treatment, even if the direct medication cost is higher.
| Insurance and cost considerations:
• Under mental health parity laws, most insurance plans must cover MAT medications • Both Sublocade and Suboxone are covered by the majority of commercial insurance plans • Medicaid coverage for Sublocade varies by state, our team can verify your specific coverage • Manufacturer patient assistance programs exist for both medications for eligible patients • Generic buprenorphine/naloxone significantly reduces Suboxone costs for cash-pay patients |
Withdrawal and Stopping Treatment Safely
One of the most important, and most misunderstood, aspects of buprenorphine-based MAT is what happens when treatment ends. Both Sublocade and Suboxone produce physical dependence: the body adapts to the presence of buprenorphine, and stopping abruptly causes withdrawal. This is a predictable physiological consequence of any opioid receptor modulator, and it is manageable with proper medical supervision.
Suboxone Withdrawal
Suboxone withdrawal, when it occurs, is typically less severe than withdrawal from full opioid agonists, but it should not be minimized. Symptoms can include muscle aches, insomnia, anxiety, irritability, nausea, sweating, and dysphoria. The timeline and severity depend significantly on the dose and duration of use.
When discontinuing Suboxone, the standard clinical approach is a gradual taper, slowly reducing the dose over weeks to months to allow the body to adjust incrementally. This taper should always be physician-supervised. Stopping Suboxone abruptly is rarely clinically appropriate and carries meaningful risk of relapse.
Sublocade Withdrawal
Because Sublocade releases buprenorphine gradually and its blood levels decline slowly after the last injection, withdrawal symptoms following discontinuation of Sublocade are typically more gradual in onset and often less acute than those following abrupt cessation of oral buprenorphine. The natural taper built into the pharmacokinetics of the depot formulation provides some protection against the sharpest withdrawal symptoms.
“Stopping buprenorphine treatment prematurely is one of the most significant risk factors for opioid relapse. The decision to discontinue MAT should always be made collaboratively, carefully, and with a full clinical plan in place.”
Who Is the Ideal Candidate for Each?
The most clinically useful way to think about Sublocade versus Suboxone is not as competing medications, but as tools designed for different moments in the recovery journey and different patient profiles. The comparison below is a clinical starting point, never a substitute for an individualized assessment with your treatment provider.
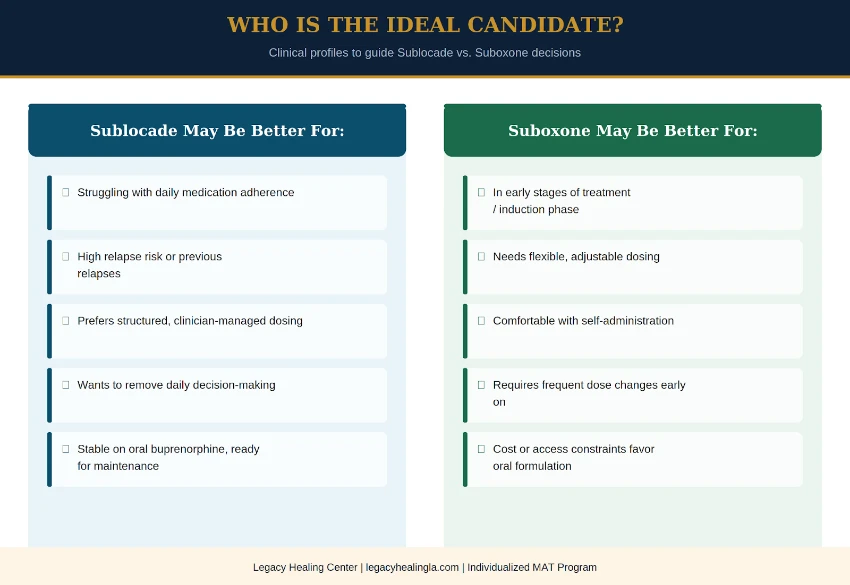
It is worth noting that many patients begin their MAT journey on Suboxone and later transition to Sublocade as their recovery stabilizes, and this is a common and clinically supported progression.
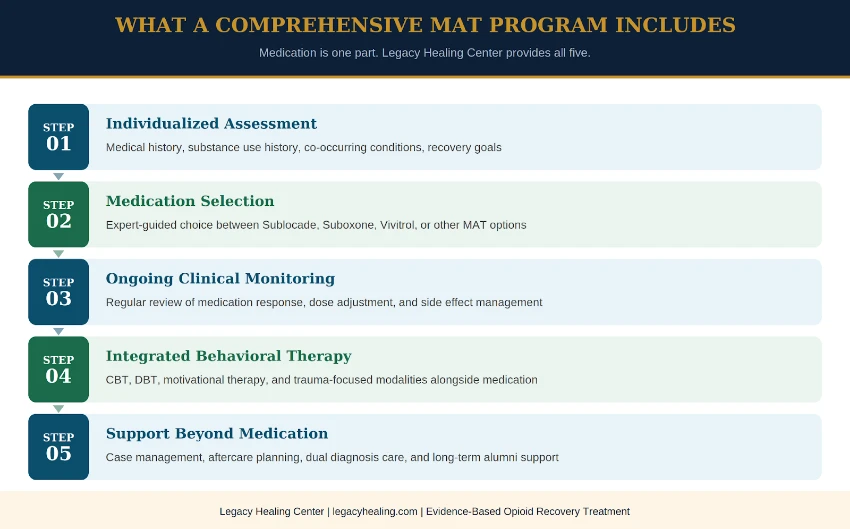
Finding the Right Medication-Assisted Treatment Program
The medication is only one part of what makes MAT work. The program around the medication, the clinical oversight, the therapy integration, the support structures, is equally important, and in many ways more determinative of long-term outcomes.
Legacy Healing Center’s medication-assisted treatment program is built around a simple clinical principle: medication manages the physiology; therapy and support address the full human experience of recovery. Neither alone is sufficient. Both together are powerful.
The Decision That Belongs to You, Made With Expert Support
Choosing between Sublocade and Suboxone is not a decision that should be made alone, or based solely on what you have read online, including this article. It is a clinical decision that should be made in partnership with an addiction medicine specialist who knows your history, understands your recovery goals, and has the expertise to recommend the option most likely to work for you specifically.
Our medical team is available to answer your questions, conduct a confidential assessment, and help you understand which MAT pathway makes the most sense for where you are in your recovery.






